Asymptomatic carriers presenting a high-risk antiphospholipid antibody profile.
Antiphospholipid antibodies (aPLs) constitute a heterogeneous group of auto- antibodies associated with thrombosis related events, and define the anti-phospholipid syndrome (APS) (22). APS is an autoimmune disease characterized by venous or arterial thrombosis and/or obstetric complications. Clinical criteria associated with the persistent positivity of at least one aPL, such as Lupus Anticoagulant (LA) or antibodies directed against Cardiolipin (aCL) or β2-Glycoprotein I (aβ2GPI) of IgG or IgM isotype, is necessary for APS diagnosis (6). Functional tests, based on clotting time are used for the detection of LA, described as the most correlated marker to clinical manifestations (30). APS mainly affecting young people, is a severe disease, which requires long-term anticoagulant therapy, and despite this, thrombotic recurrences are frequent. aPLs are not only used for APS diagnosis, they also have an important role in the pathophysiology of the disease. A two hit hypothesis has been suggested to explain why thrombotic events occur only occasionally in spite of the persistent presence of autoantibodies (22). aPL (first hit) increase the thrombotic risk and clot takes place in the presence of another thrombophilic condition, such as infectious or inflammatory diseases (second hit) .
It is now widely recognized that multiple positivity of aPL is more frequently associated with thrombotic or obstetrical events than single one (38, 41). Pengo et al demonstrated that among multiple positivity, triple positivity which is defined as the association of LA, aCL and aβ2GPI, irrespective of their isotype, represents the aPL profile associated with the highest risk of thromboembolic events occurrence and severe pregnancy morbidity (64). However, triple positivity is also described in asymptomatic “carriers” raising the dilemma of whether to initiate or not a primary thromboprophylaxis. To better stratify the thrombotic risk, an appropriate interpretation of aPL positivity has been challenging. To this end, we performed a retrospective study on 7111 samples to select triple positive patients presenting or not thrombotic related events. Among them a comparison was made between.
Material and methods
7111 samples were tested, corresponding with 6500 patients. Subjects were grouped according to their laboratory profile. We considered LA positive if at least one of the two tests performed was positive (PTT-LA and dRVVT), aCL or aβ2GPI positive if IgG or IgM isotype test detection was positive. We obtained 528 patients with a single test positive (208 LA positive, 157 aCL positive and 163 aβ2GPI positive), 116 patients double positive (33 LA & aβ2GPI positive, 38 LA & aCL positive, and 45 aCL and aβ2GPI positive) and 93 triple positive patients (Fig. 1). venous or arterial thromboembolism (such as deep vein thrombosis, pulmonary embolism, stroke, transient ischemic attack, myocardial infarction); (ii) history of obstetrical complications; (iii) clinical manifestations not included in revised criteria (6); (iv) arterial risk factors (smoking habit, hypercholesterolemia, high blood pressure, diabetes, obesity, family history), (v) venous risk factors (combined oral contraceptive, pregnancy, neoplasia, thrombophilia, family history). NB: Concerning « family history » we were looking for: history of venous thromboembolism (VTE) in first-degree relative (parent or sibling); or history of myocardial infarction or sudden cardiac death in a first-degree relative men younger than 55 years old or in a first-degree relative women younger than 65 years old; or history of stroke in a first degree relative (parent or sibling) before 45 years old.
Furthermore, we systematically collected those biological data : (i) persistence of aPL; (ii) persistence of triple positivity; (iii) presence (or absence) of antinuclear antibodies; (iv) presence (or absence) of anti-DNA; (v) ABO blood group status, considering only “O blood groups” versus “non-O blood groups”, since it is well established that O blood group status is a risk factor for thrombosis (75), (vi) platelets, (vii) hemoglobin, with Mean Corpuscular Volume (MCV) and Mean Corpuscular Hemoglobin Concentration (MCHC), (viii) white blood cells and neutrophils, (ix) bilirubin, LDH and haptoglobin, to evaluate a potential hemolysis. of Thrombosis and Haemostasis (ISTH) using two clotting times: Partial Thromboplastin Time- Lupus Anticoagulant (PTT-LA) by STAGO® and diluted Russel Viper Venom Time (dRVVT) by STAGO®. We calculated the Rosner Index (RI) and we considered positive when RI > 15. Results of dRVVT were expressed with a Normalized Ratio (NR) (positive value, > 1.2).
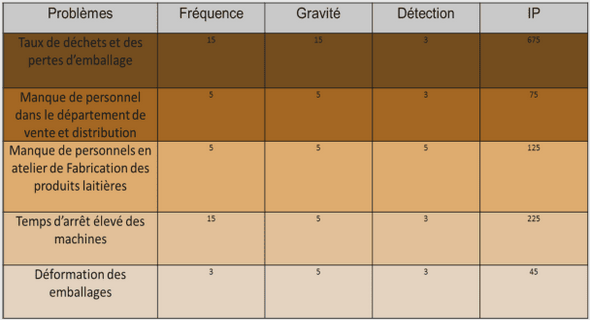
Over a 2-year period, we selected 93 patients presenting a triple positivity, defined as the association of LA, IgG and/or IgM aCL, and IgG and/or IgM aβ2GPI. Among them, 5 patients were excluded according to criteria as defined in material and methods. As shown in Table 1, we constituted two groups of patients based on their clinical history. compared by Student’s t test and categorical data by the χ² test or Fisher test. Estimation of odds ratio for each variable was calculated using univariate logistic regression. Variables with p-values < 0.20 were considered as candidates for the multivariate analysis. For multivariate analysis, we considered two or most cardiovascular risk factors (including high blood pressure, diabetes, obesity, dyslipidemia, smoking habit, combined oestroprogestative contraceptive and age older than 45 years old). All tests were two-sided. p<0.05 was retained for significance.